

 Osteoporosis is common in the United States. It is estimated that approximately 10% of the population 50 years and older have osteoporosis in the U.S.1 This equates to millions of Americans having “weak” bones putting them at risk for a fracture.
Osteoporosis is common in the United States. It is estimated that approximately 10% of the population 50 years and older have osteoporosis in the U.S.1 This equates to millions of Americans having “weak” bones putting them at risk for a fracture.
Osteoporosis can be prevented, and even treated, with diet and lifestyle changes. You can learn more about this topic by reading my previous article – Osteoporosis – The Diet and Lifestyle Connection.
In this article, I want to focus on medications and supplements used to treat osteoporosis. I will review what types of medications and supplements are used to treat osteoporosis, the success rates of these medications, and their potential side effects.
A Quick Lesson In Statistics and Reported Success Rates
Before proceeding, it’s important for you to understand how statistics are reported. By doing so, you’ll see how easy it is to be misled by the advertising and marketing campaigns of pharmaceutical companies trying to sell you their drug or supplement. I’m not saying that pharmaceutical drugs don’t work. They just don’t work as well as we’ve been led to believe most of the time. It’s beneficial for you to know this and to understand the story behind the story.
 Most studies (and advertisements) report success rates in terms of relative risk reduction. This falsely elevates the “success rate” of any drug or supplement. The relative risk reduction only takes into account study participants who experience an event.
Most studies (and advertisements) report success rates in terms of relative risk reduction. This falsely elevates the “success rate” of any drug or supplement. The relative risk reduction only takes into account study participants who experience an event.
For example, let’s say I have a drug used to treat osteoporosis. The goal of using my drug is to prevent fractures in patients. The study consists of 200 participants, divided equally into two groups (100 in the drug group and 100 in the placebo group). After three years of taking the drug/placebo here are the results:
- Drug group = 2 fractures [2 out of 100 people (2%) in this group experience a fracture]
- Placebo group = 4 fractures [4 out of 100 people (4%) in this group experience a fracture]
The relative risk reduction or “success rate” is a 50% reduction in fractures. How do they come up with this?
Two is half of four. Therefore, this is a 50% reduction in the risk of experiencing a fracture in those taking the drug versus those taking the placebo. This is the relative risk reduction.
- Relative risk reduction ⇒ 2 ÷ 4 = 50%
However, there were more than six people in the study. There were 200 people in fact, 100 in each group. If you forget about the other 194 people who did not experience a fracture, and only focus on the six people who did, then there really is a 50% reduction in fracture risk.
But, if you wish to include the other 194 people who did not experience a fracture, then the success rate is actually only a 2% reduction in fracture risk. This is called the absolute risk reduction (ARR). It is calculated by taking the difference between the fracture rates between the two groups.
- Absolute risk reduction ⇒ 4% – 2% = 2%
That’s a big difference! Not all drugs have such a big difference between the relative and absolute risk reduction, but you need to know what these terms mean and where they come from.
Another way to express success rates in clinical studies is to use the number needed to treat (NNT). The NNT is simply the number of people needed to treat over a specified amount of time with the drug to prevent one bad outcome (i.e. fracture). For example, in our sample problem above the NNT is 50. Fifty people would be need to be treated for three full years in order for one person to benefit from taking the drug.
The NNT is calculated using the ARR. Like ARR, it gives a more realistic view of how well a medication works when including all of the study participants in the calculated results. The NNT allows you to view the success rate from a different angle. It gives you a big picture view of the clinical trial.
Please see below to understand how the NNT is calculated. Remember that 2% is the same thing as 0.02 which is our ARR in our sample problem.
- NNT = 1 ÷ ARR
- Calculating NNT from our example above ⇒ NNT = 1 ÷ 0.02 = 50
It isn’t important that you memorize how the NNT is calculated. It’s just important that you understand what it means so you can put it into perspective as you read the results of various osteoporosis drugs later in this article.
Medications Used to Treat Osteoporosis
 There are several supplements and medications used to treat osteoporosis. They are divided up into different classes below. When available, I will report success rates in terms of ARR rates and numbers needed to treat (NNT).
There are several supplements and medications used to treat osteoporosis. They are divided up into different classes below. When available, I will report success rates in terms of ARR rates and numbers needed to treat (NNT).
Supplements
The most common supplements used to treat osteoporosis are calcium and vitamin D. Many times these are taken together in the same pill. So how well do they work?
Calcium
How it works – Calcium is the major mineral within the bone. The human body stores 99% of its calcium in our bones.2 Calcium is necessary in the formation of bone, along with phosphorus, but we tend to go overboard when it comes to consuming or supplementing with calcium. For a more in depth look at this topic please read my article – The Calcium Myth – More Is Not Better.
Success rate – A 2015 systemic review of calcium intake and fracture risk published in the British Medical Journal concluded the following on this topic – “In summary, our analyses indicate that dietary calcium intake is not associated with risk of fracture, and there is no evidence currently that increasing dietary calcium intake prevents fractures. Calcium supplements have small inconsistent benefits on fracture reduction but probably have an unfavourable risk:benefit profile. There was no risk reduction in fracture at any site in pooled analyses of the randomised controlled trials of calcium supplements at lowest risk of bias, and there was evidence of publication bias in small-moderate sized trials. Collectively, these results suggest that clinicians, advocacy organisations, and health policymakers should not recommend increasing calcium intake for fracture prevention, either with calcium supplements or through dietary sources.”3
Potential side effects (no frequency defined) – Anorexia, constipation, low blood pressure, headache, flatulence, nausea, vomiting, low phosphate and/or magnesium levels4,5
Vitamin D
How it works – Vitamin D works to regulate bone formation and also regulates calcium and phosphorus absorption in the gut.6 For information on supplementing with vitamin D please read my article – Vitamin D – To Supplement or Not to Supplement.
Success rates7
- Vitamin D ARR in preventing fractures (older adults in the community) – 0%
- Vitamin D ARR in preventing fractures (elderly adults, nursing home) – 2.8% (NNT=36)
Potential side effects – Kidney stones or kidney damage (2.8%)7,8. For more information on mortality data (i.e. death rates) while taking vitamin D please read my article – How to Feel Vitamin “D”errific!
Bisphosphonates
The bisphosphonates are typically the first class of prescription drugs used by physicians and their patients to treat osteoporosis. They come in injectable and oral dosage forms. The bisphosphonates include Fosamax (alendronate), Actonel/Atelvia (risedronate), Boniva (ibandronate), and Reclast (zolendronic acid).
How they work – Bisphosphonates work by inhibiting osteoclast activity.9 Remember, osteoclasts are the cells that consume or breakdown old bone to make way for new. Bisphosphonates prevent the breakdown of old bone.
Success rates10
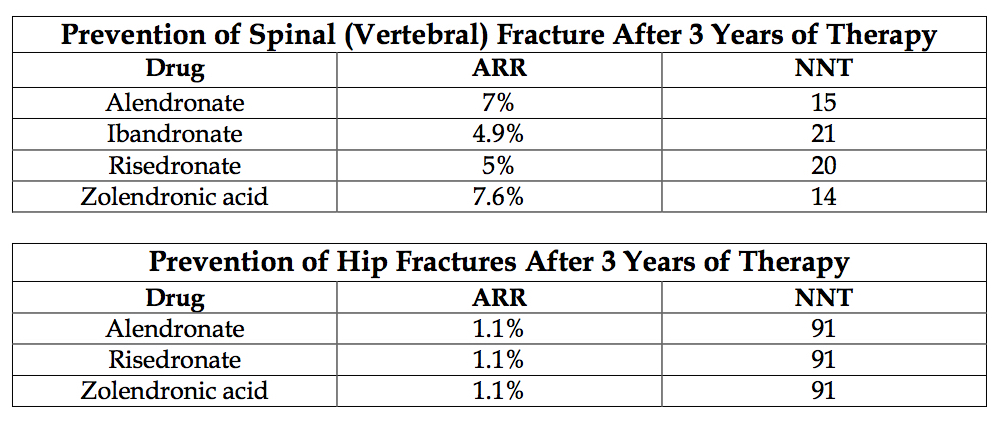
Potential side effects
The side effects listed here are for Fosamax (alendronate), which is one of the most common medications used in this class.11 For side effects of other bisphosphonates please visit the Medscape pages for risedronate, ibandronate, and zolendronic acid.
Fosamax side effects
Low calcium blood levels (18%)
Low phosphorus blood levels (10%)
Abdominal pain (7%)
Musculoskeletal pain (4.1%)
Indigestion (3.6%)
Nausea (3.6%)
Constipation (3.1%)
Diarrhea (3.1%)
Flatulence (2.6%)
Headache (2.6%)
Acid reflux (2%)
Inflammation of the esophagus (1.5%)
Abdominal distention (1%)
Estrogen Receptor Stimulators
Estrogen and Evista (raloxifene) are the two main medications used in this class of drugs. These are not first-line therapy options for osteoporosis, but instead used after bisphosphonate or other drug therapies due to their potential risks.
How they work – This group of drugs works by decreasing osteoclast activity, which results in less old bone being broken down and disposed of.9 Estrogen can also play a small role in increasing calcium absorption in the body.
Success rates9,10
- Estrogen ARR in preventing hip fractures in postmenopausal women – 0.46% (NNT=216)
- Estrogen ARR in preventing spine fractures in postmenopausal women – 0.44% (NNT=225)
- Raloxifene ARR in preventing spine fractures after 3 years of therapy – 3.4% (NNT=29)
Potential side effects9,12,13
Estrogen has been reported to increase strokes by 0.8% and blood clots by 0.45%. More side effects for estrogen and raloxifene are listed below.
Conjugated estrogen (Premarin) side effects
Abdominal pain (15-17%)
Back pain (13-14%)
Breast enlargement/breast tenderness (7-12%)
Headache (26-32%)
Arthralgia (7-14%)
Sore throat (10-12%)
Sinus infection (6-11%)
Diarrhea (6-7%)
Depression (5-8%)
Dizziness (4-6%)
Nervousness (2-5%)
Flatulence (6-7%)
Vaginal inflammation (5-7%)
Vaginal discharge (4-7%)
Leg cramps (3-7%)
Increased cough (4-7%)
Severe itching of the skin (4-5%)
Raloxifene side effects
Hot flashes (8-29%)
Flu syndrome (14-15%)
Cramps/muscle spasm (6-12%)
Arthralgia (11-16%)
Infection (11%)
Insomnia (6%)
Vomiting (5%)
Sinus infection (10%)
Bronchitis (10%)
Sore throat (8%)
Breast pain (4%)
Stomach flu (<3%)
Sweating profusely (3%)
Blood clots (1-2%)
Calcitonin
Calcitonin is known by the brand names Miacalcin or Fortical. It is derived from animal protein, usually salmon. Calcitonin comes in a nasal spray and an injectable form.
How it works – Calcitonin works primarily by decreasing osteoclast activity, thereby inhibiting the breakdown of old bone.9
Success rate9
- Calcitonin ARR in preventing spine fractures after 5 years of therapy – 3% (NNT=33)
Potential side effects14
Runny/stuffy nose (12%)
Arthralgia (4%)
Back pain (5%)
Nose bleeds (4%)
Injection site reactions (10%)
Nausea (10%)
Headache (3%)
Flushing of face or hands (2-5%)
Denosumab (Prolia)
Denosumab, known better by its brand name Prolia, is an injectable drug given twice a year to prevent osteoporotic fractures.
How it works – Denosumab works by inhibiting osteoclast activity, which reduces the breakdown of old bone and prevents bone turnover.15
Success rate16
- Denosumab ARR in preventing spine fractures after 3 years of therapy – 5.3% (NNT=19)
- Denosumab ARR in preventing non-vertebral fractures (hip, wrist, ankle, rib) after 3 years of therapy – 1.4% (NNT=71)
Potential side effects17
Back pain (34.7%)
Extremity pain (11.7%)
Musculoskeletal pain (7.6%)
High cholesterol levels (7.2%)
Inflammation of the bladder (5.9%)
Upper respiratory tract infection (4.9%)
Sciatica (4.6%)
Nonfatal serious infection (4%)
Bone pain (3.7%)
Anemia (3.3%)
Upper abdominal pain (3.3%)
Rash (2.5%)
Flatulence (2.2%)
Osteonecrosis of jaw (2.2%)
Severe itching of the skin (2.2%)
Low blood calcium levels (1.7%)
Teriparatide (Forteo)
Teriparatide, known by its brand name Forteo, is a daily injectable drug used to prevent fractures from osteoporosis. The manufacturer of Forteo recommends to limit the use of this drug to no more than two years over a person’s lifetime due to a lack of safety and efficacy beyond this timeframe.
How it works – Teriparatide works by regulating calcium and phosphorus absorption and excretion in the body. It also increases osteoblast cell activity in the bones, which increases new bone formation.9
Success rate10
- Teriparatide ARR in preventing spine fractures after 3 years of therapy – 9% (NNT=12)
Potential side effects18
High calcium blood levels (transient increases 4-6 hours after dose; 11% of women, 6% of men)
Arthralgia (10%)
Stuffy/runny nose (10%)
Nausea (9%)
Weakness (9%)
Dizziness (8%)
Sore throat (6%)
Indigestion (5%)
Rash (5%)
Depression (4%)
Difficulty breathing (4%)
Pneumonia (4%)
Vertigo (4%)
Antibodies to teriparatide (3% of women in long-term treatment)
Chest pain (3%)
High uric acid blood levels (3%)
Leg cramps (3%)
Syncope (fainting) (3%)
Vomiting (3%)
Tooth disorder (2%)
Conclusion
As you can see, there are many different types of supplements and drugs used to treat osteoporosis. All of them have potential benefits and risks that you need to evaluate before taking. Talk these items over with your doctor and/or pharmacist if you need to. Remember, ultimately it is your body and your life that you are making a decision on. You are in charge of the choices you make regarding your health, and you have to live with them good or bad. There is no right or wrong decision when it comes to your health, just different possibilities to consider. Being informed goes a long ways in helping you make smart decisions.
Don’t forget to always make a healthy, plant-based diet and regular exercise part of your everyday choices. Both have been proven to help osteoporosis regardless of whether or not you choose to take medication to treat your condition. As a bonus, positive diet and lifestyle choices also improve other chronic conditions like heart disease and obesity too. It is truly a win-win situation.
Stay healthy and be informed!
Related articles:
Osteoporosis – Screening Bones For Answers to Your Health
Osteoporosis – The Diet and Lifestyle Connection

.jpg "The Empty Medicine Cabinet")
If you like what you see here, then you’ll LOVE my daily Facebook and Twitter posts! Also, don’t forget to sign up for my Free Online Mailing List to get all the latest updates from the Plant-Based Pharmacist!
Check out my book, The Empty Medicine Cabinet, to start your journey towards better health. This step-by-step guide leads you through many of today’s common chronic diseases (heart disease, obesity, diabetes, cancer, and more), giving you the facts on food versus medication in treating these medical conditions. The book also contains an easy-to-follow guide on how to adopt a whole foods, plant-based diet as a part of an overall lifestyle change, producing the best possible health outcomes for you and your family. Hurry and get your copy today!
References:
1 Wright NC, Looker AC, Saag KG, et al. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J Bone Miner Res. 2014 Nov;29(11):2520-6.
2 Flynn A. The role of dietary calcium in bone health. Proc Nutr Soc. 2003 Nov;62(4):851-8. Review.
3 Bolland MJ, Leung W, Tai V, et al. Calcium intake and risk of fracture: systematic review. BMJ. 2015 Sep 29;351:h4580.
4 Calcium Carbonate Adverse Effects. Medscape. Available: http://reference.medscape.com/drug/tums-calcium-carbonate-341983#4. Accessed 15 Aug 2016.
5 Calcium Citrate Adverse Effects. Medscape. Available: http://reference.medscape.com/drug/citracal-calcium-citrate-999216#4. Accessed 15 Aug 2016.
6 Bikle DD. Vitamin D and Bone. Current osteoporosis reports. 2012;10(2):151-159.
7 Newman D. Vitamin D For Preventing Fractures (Older Adults in the Community). 15 May 2011. Available: http://www.thennt.com/nnt/vitamin-d-for-fracture-prevention-community/. Accessed 15 Aug 2016.
8 Newman D. Vitamin D for Preventing Fractures (Elderly, Institutionalized Adults). 15 May 2011. Available: http://www.thennt.com/nnt/vitamin-d-for-fracture-prevention-elderly-nursing-home/. Accessed 15 Aug 2016.
9 MacLaughlin EJ, Sleeper RB, McNatty D, Raehl CL. Management of Age-Related Osteoporosis and Prevention of Associated Fractures. Therapeutics and Clinical Risk Management. 2006;2(3):281-295.
10 Ringe JD, Doherty JG. Absolute risk reduction in osteoporosis: assessing treatment efficacy by number needed to treat. Rheumatol Int. 2010;30:863-869.
11 Alendronate Adverse Effects. Medscape. Available: http://reference.medscape.com/drug/fosamax-binosto-alendronate-342810. Accessed 16 Aug 2016.
12 Conjugated estrogens Adverse Effects. Medscape. Available: http://reference.medscape.com/drug/premarin-estrogens-conjugated-342771#4. Accessed 16 Aug 2016.
13 Raloxifene Adverse Effects. Medscape. Available: http://reference.medscape.com/drug/evista-raloxifene-342794#4. Accessed 16 Aug 2016.
14 Calcitonin Adverse Effects. Medscape. Available: http://reference.medscape.com/drug/fortical-miacalcin-calcitonin-salmon-342816#4. Accessed 16 Aug 2016.
15 Hanley DA, Adachi JD, Bell A, Brown V. Denosumab: mechanism of action and clinical outcomes. Int J Clin Pract. 2012 Dec;66(12):1139-46.
16 Papapoulos S, Lippuner K, Roux C, et al. The effect of 8 or 5 years of denosumab treatment in postmenopausal women with osteoporosis: results from the FREEDOM Extension study. Osteoporos Int. 2015 Dec;26(12):2773-83.
17 Denosumab Adverse Effects. Medscape. Available: http://reference.medscape.com/drug/prolia-denosumab-999566#4. Accessed 16 Aug 2016.
18 Teriparatide Adverse Effects. Medscape. Available: http://reference.medscape.com/drug/forteo-teriparatide-342831#4. Accessed 16 Aug 2016.
Pingback: Osteoporosis – The Diet & Lifestyle Connection - Plant-Based Pharmacist
This is extremely helpful information for someone like me who has just been prescribed fosamax. Have you done a chart of other common drugs that show their ARRs and NNTs? In a world where there are few lifestyle doctors, it is information like this that helps people like me to make drug choices just like I make a plant-based choice every meal. Thanks
Pingback: Osteoporosis – Screening Bones For Answers to Your Health